Tom and Terri Collura
BrainMaster Technologies, Inc.
In this discussion we will address some of the clinical, technical, and medicolegal aspects of remote training. Fundamentally, remote training consists of sending EEG neurofeedback equipment into the home, school, or office, where it is used in the absence of direct supervision of the responsible clinician. We are seeking a new model, in which the EEG instrument becomes more like an electronic dispenser, that administers treatments according to specific protocols and parameters set by a supervising clinician, and administered in a remote location (home, school, office). We seek provisions that ensure that the clinician has access to ongoing information regarding the progress of training, and maintains a level of control sufficient to ensure the quality and effectiveness training, without the need to be physically present during all training sessions.
There are certain barriers to effective remote neurofeedback that must be cleared, if progress is to be made. It is an unavoidable fact that neurofeedback is a procedure that requires clinical supervision, and that the requisite equipment is regarded as a prescription device. Moreover, the clinician is responsible for the conduct and results of neurofeedback training, even if sessions are not conducted in the office. Finally, it is clear that remote neurofeedback will not gain the acceptance it needs, unless there is a way to ensure that quality is assured, even when equipment leaves the office.
Remote neurofeedback training should not consist of simply sending a clinical instrument home with a trainee, while expecting a parent, companion, or the trainee themselves to become a neurofeedback therapist. Rather, the remote-based system should have a level of simplicity and control that makes it easy to use, while ensuring compliance. The clinician requires ongoing indications of the progress of treatment, the time, duration, and outcome of individual sessions, EEG changes, behavioral notes, and so on. The key necessity is that clients can easily perform the training that has been defined, and that the clinician can be made quickly aware of how things are progressing, and has the ability to make changes as necessary.
We believe that in order for neurofeedback to reach the next level of acceptance and deployment, costs must be decreased, and time in the clinic must be reduced. We see the conventional series of 40 in-office visits at $50 to $100 apiece, being replaced by a small number of in-office training sessions, which punctuate the remote training. We seek a new way of looking at equipment, software, and clinical activities, which will help to transform neurofeedback from a primarily clinic-based activity into one that can be conducted any time, any where, while maintaining a level of clinical supervision and confidence that sufficiently approximates what can be achieved in the clinic.
If we can achieve these goals, the following realities may come to pass:
- A reduction in the cost of a typical neurofeedback regimen from the current level of $2000-$4000, to $500-$1000. This will have a profound effect on the attitudes of insurance providers, schools, parents, and other entities that bear the financial burden of the training.
- An increase in the number of clients that a given practitioner can serve, from 20-40, to 100 or more.
- A shift in the professional and financial picture of clinical neurotherapy, in which charges for professional services, equipment rental, remote supervision, and ongoing assessment supplement or replace the usual office visits, making the clinical task less labor-intensive, and more cognitive in nature.
- A broadening of the client base of all clinicians, who now can overcome geographical and financial barriers, as they serve a wider range of clients than ever before.
- An increased awareness and acceptance of neurofeedback, as more clients are able to afford training, and reap the benefits.
Many practitioners believe that effective remote training requires some form of real-time connectivity, so that the training session(s) can be monitored live, to ensure that all is necessary is to ensure that the training is proceeding as planned, but this can be managed by a system that allows the supervising clinician to see results, review self-assessments and related reports, and discuss progress over the telephone. Indeed, one of the more active clinicians we know has more than 30 EEG systems in the field, in various states, some thousands of miles from the office. All clients must being with an in-office orientation and training, and then proceed to a home-based training program, in which geographical distance is not so much of an issue.
While this practice has been successful so far, it clearly taxes the abilities of clinicians and trainees, as well. Home users are obligated to learn to use equipment according to the same procedures as a clinician, including setting up the protocols, managing thresholds, monitoring progress, reviewing summary information, and determining whether the progress is satisfactory. We seek to relieve much of this burden on both sides, while ensuring the quality and effectiveness of remote training.
Overall, we see the use of home/school/office EEG increasing 10-fold or more, as a result of simple, yet crucial changes in how we approach the total set of issues.
To these ends, we see the following components as being critical to the effectiveness of remote training:
- Provisions for clinicians to design protocols and sessions on one system, that can be conducted on another system.
- Means to convey protocol and session settings to the remote system via inexpensive and simple means (email, floppy disk, internet, etc). This should include a method for remote trainees to incorporate this information into their system in a simple, fail-safe manner.
- Means to ensure that remote trainees are limited to the prescribed activities, and cannot go outside the boundaries that have been defined. This should also include a means to ensure that trainees have actually conducted the prescribed training, for the recommended times and durations, and that the resulting EEG data reflect appropriate changes.
- Means to convey results to the clinician, again via inexpensive and simple means (email, floppy disk internet, etc). Results should include general session data (time, duration, etc), training results (points scored, percent rewards, etc), specific EEG results (amplitudes, etc), and associated self-report and behavioral data.
- Means for the clinician to review training results, make changes when indicated, and convey these changes back to the remote location.
Based on a focus on these simple requirements, it is possible to configure systems that effectively address remote training needs, without increasing their complexity or cost. Indeed, it is possible to produce home-based systems that are considerably affordable, with an initial capital cost of $1000 or less, and that can be leased, loaned, or otherwise allotted to remote trainees who do not have to bear the purchase cost of equipment. Overall, we see it possible for remote trainees to subscribe to “pay as you go” plans, in which EEG training is made available for on the order of $100 or $300 a month, thus reaching a considerably enlarged client base, while providing effective, quality training.
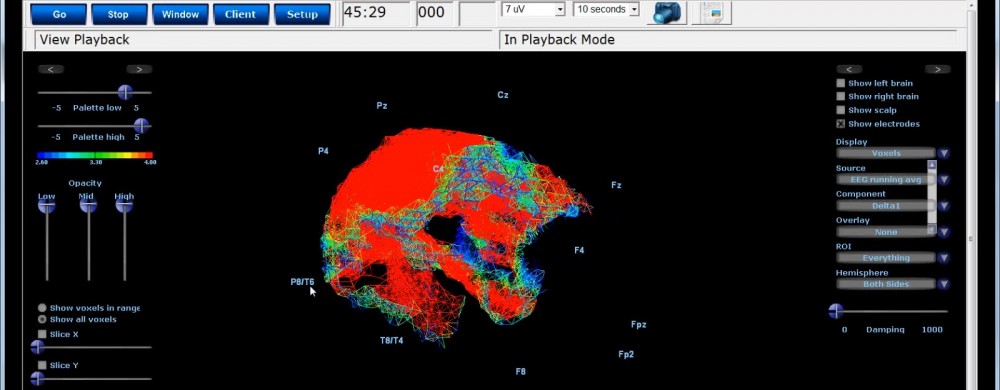

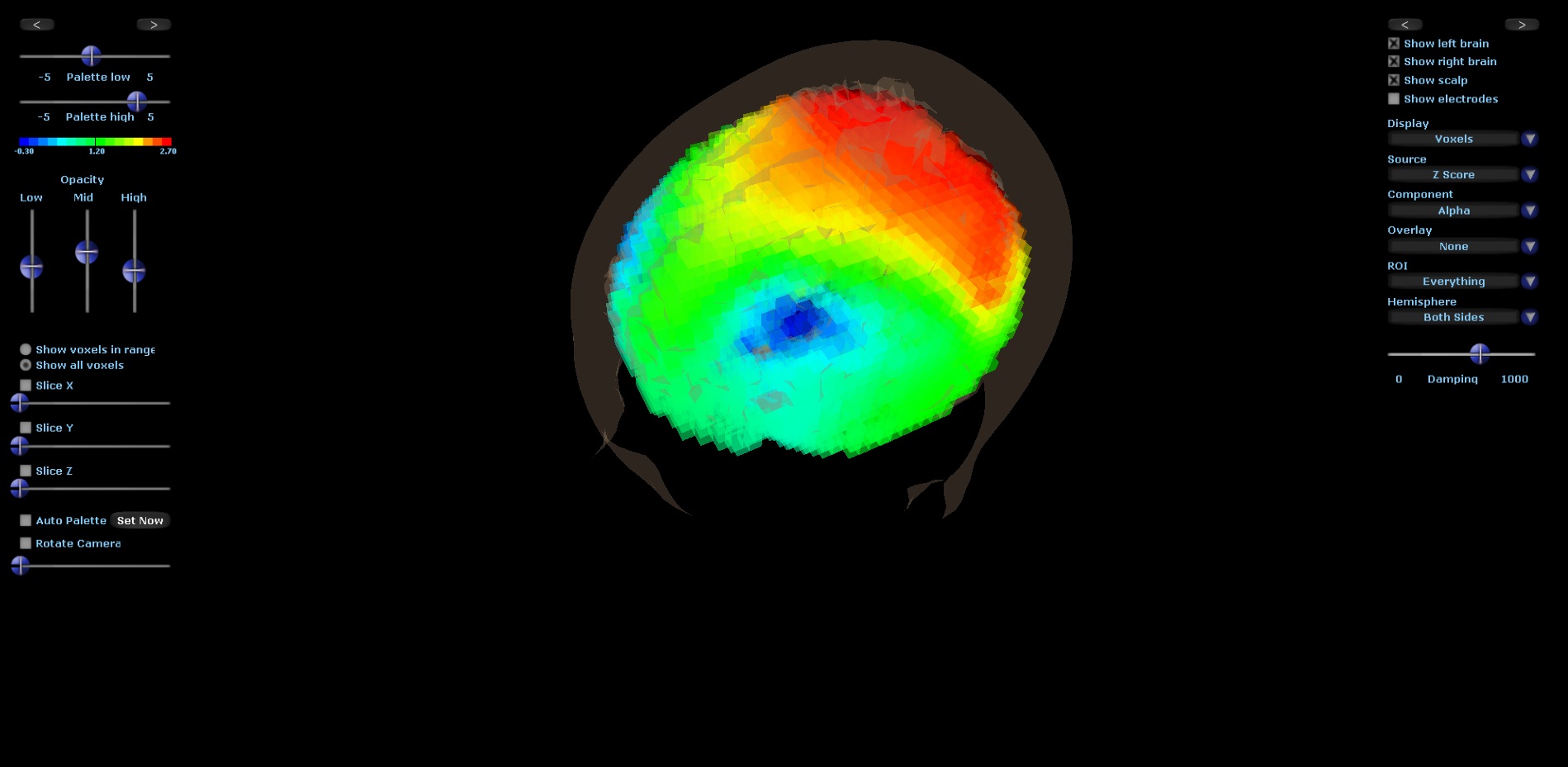 The attached talk was presented at the 27th Annual Psychological Trauma Conference in Boston on June 2, 2016. These results show brain activation patterns that found in individuals experiencing traumatic and emotionally charged stimulation and experiences. We find that the responses of the frontal lobes demonstrate specific positive and negative emotional responses, and underlie decision-making processes. The frontal hemispheres are lateralized, in that the left hemisphere and right hemisphere perform different functions, and that both are necessary for healthy, flexible, adaptable responses. Depending on past experiences, particularly trauma, this balance of reactivity may be affected. The left hemisphere takes care of sequential, logical processing, and produces positive, or “approach” responses. The right hemisphere takes care of parallel, recognition-based responses, and produces negative, or “avoid” responses. Both of these are important, so that the individual is able to respond appropriately to positive or negative stimuli and situations. Examples are given of both adaptive, flexible responses, as well as fixed, inflexible responses. Inflexibility is associated with reactive, fixed, and maladaptive responses. Imaging an biofeedback of brain activity according to this model can be applied to counseling and other clinical activity, to help to empower and enable clients to have healthy responses, that are consistent with goals and produce beneficial mental states and behaviors.
The attached talk was presented at the 27th Annual Psychological Trauma Conference in Boston on June 2, 2016. These results show brain activation patterns that found in individuals experiencing traumatic and emotionally charged stimulation and experiences. We find that the responses of the frontal lobes demonstrate specific positive and negative emotional responses, and underlie decision-making processes. The frontal hemispheres are lateralized, in that the left hemisphere and right hemisphere perform different functions, and that both are necessary for healthy, flexible, adaptable responses. Depending on past experiences, particularly trauma, this balance of reactivity may be affected. The left hemisphere takes care of sequential, logical processing, and produces positive, or “approach” responses. The right hemisphere takes care of parallel, recognition-based responses, and produces negative, or “avoid” responses. Both of these are important, so that the individual is able to respond appropriately to positive or negative stimuli and situations. Examples are given of both adaptive, flexible responses, as well as fixed, inflexible responses. Inflexibility is associated with reactive, fixed, and maladaptive responses. Imaging an biofeedback of brain activity according to this model can be applied to counseling and other clinical activity, to help to empower and enable clients to have healthy responses, that are consistent with goals and produce beneficial mental states and behaviors.